- Visibility 26 Views
- Downloads 6 Downloads
- DOI 10.18231/j.ijor.2023.009
-
CrossMark

Is coracoid fracture with ac dislocation an unusual case
- Author Details:
-
 Dheeraj Makkar *
Dheeraj Makkar *
-
Kamik Raju Paila
Introduction
The coracoid process, a curved anterior projection of the scapula, plays a crucial role in connecting the clavicle, humerus, and scapula through various ligaments. It also serves as an attachment site for muscles. Fractures of the coracoid process are uncommon and can be challenging to detect on conventional X-rays due to their unique anatomy and alignment. Scapular fractures, including coracoid fractures, are relatively rare, accounting for a small percentage of all fractures, typically ranging from 0.4% to 1% in reported cases using plain X-rays.
According to studies using conventional X-rays, coracoid fractures represent a minority, comprising 0% to 8% of reported scapular fracture cases.[1] In this particular report, we present a unique occurrence of a coracoid process fracture along with a grade 1 acromioclavicular joint dislocation.[2] Notably, conservative treatment methods were employed and resulted in successful management of the injury.
Case Presentation
An adult male, aged 46 and working as a laborer, reported to our institute's Emergency Room with complaints of limited mobility and discomfort in the left shoulder after being involved in a road accident.



Additional symptoms included chest pain and swelling below the nipple, accompanied by ecchymosis on the anterior aspect of the left shoulder and abrasion on the posterior aspect. Physical examination revealed tenderness in the acromioclavicular joint and chest at the level of the sixth rib, along with limited range of motion in the left shoulder. Neurovascular examination of the left upper extremity was unremarkable. A plain anterior-posterior X-ray of the left shoulder revealed a grade 1 acromioclavicular dislocation ([Figure 1]), leading to suspicions of a coracoid fracture based on tenderness and X-ray findings. A chest X-ray showed a noticeable difference in the orientation of both coracoid processes, but no rib fractures were observed. Strapping was applied to the acromioclavicular joint, and a CT scan of the left shoulder was subsequently ordered.
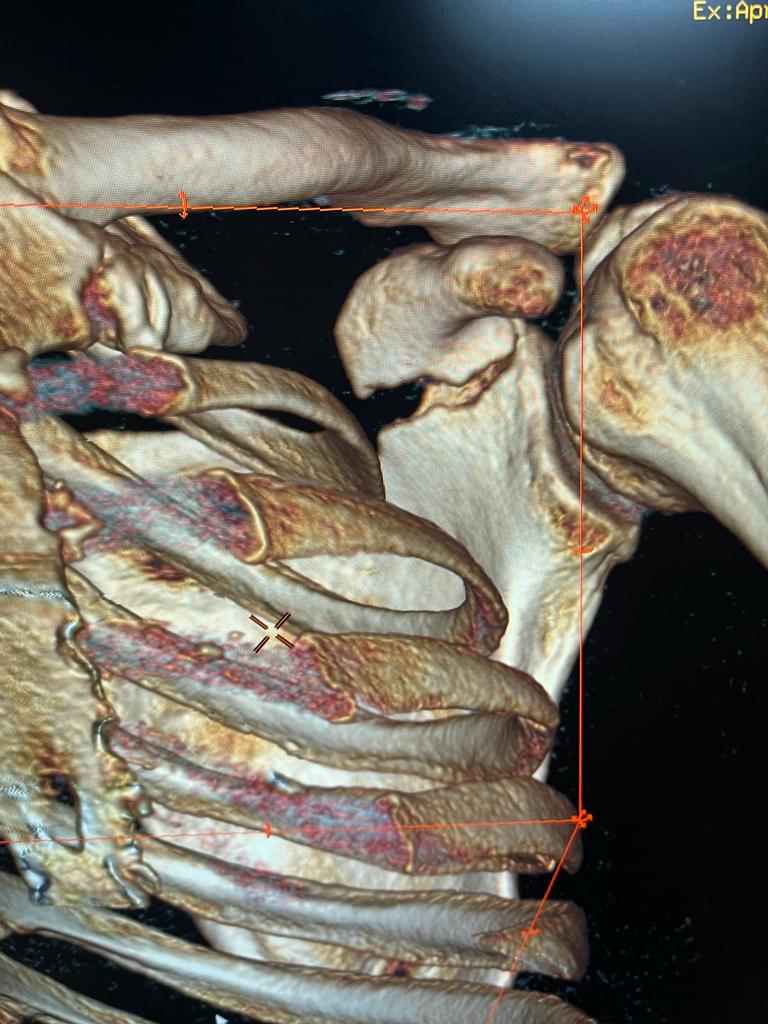
A computed tomography (CT) scan was conducted, which revealed a fracture in the sixth rib and a coracoid fracture near its base, with no involvement of the glenoid. ([Figure 2], [Figure 3]) The maximum distance between the fractured fragments was measured at 3mm, which was categorized as Ogawa type 2. Conservative treatment was chosen, and the patient was provided with a sling and acromioclavicular dislocation strapping. Follow-up X-rays were taken a week later to assess displacement between the fractured fragments, which confirmed the coracoid was in an acceptable position. Subsequent radiographs were taken at three and six weeks following the incident, with the six-week radiograph confirming union of the fracture ([Figure 4]). The patient was started on passive range of motion exercises followed by active exercises, and after three months of follow-up, he had a normal range of motion.
Discussion
Fractures involving the coracoid process are uncommon, comprising approximately 1% to 3% of all shoulder fractures. They can be classified into two main categories: fatigue fractures and traumatic fractures, with the latter being the most prevalent. Activities such as golfing, trap shooting, and cricket that involve repetitive movements make individuals more susceptible to fatigue fractures. Motor vehicle accidents are the primary cause of traumatic fractures, followed by falls from height, sports-related injuries, and heavy objects impacting the shoulder.[3] Traumatic fractures can occur as a result of direct impact, collision with a dislocated anterior humeral head, or indirect damage caused by tendon or ligament insertion. Direct impact typically leads to fractures at the base of the coracoid process, with such fractures commonly observed around the ossification site in adolescents.
Ogawa and colleagues have classified coracoid fractures into two types based on their relationship to the coracoclavicular ligament.[3] Type 1 fractures occur anterior to the ligament, whereas type 2 fractures occur posteriorly.[4] Type 1 fractures are the most prevalent, accounting for 77% of all coracoid fractures, while type 2 and traction fractures constitute 19% and 5%, respectively. Traction fractures typically occur in adolescents at the physis. In the presented case, the patient experienced an Ogawa type 2 fracture.[3]
Coracoid fractures can be challenging to diagnose due to their anatomical location, and type 2 fractures are more prone to being missed.[5] Delayed diagnosis can result in complications such as non-union, pain during shoulder joint movement, instability, and difficulty in performing daily activities. In such cases, surgical intervention is necessary to achieve union. Therefore, specialized shoulder radiographs like scapula Y or lateral and axillary views should be obtained to rule out a coracoid fracture. Surgery is the recommended treatment option for coracoid fractures in certain populations, including manual laborers and athletes.[6] Surgical fixation can be performed through open approaches using an anterior or posterior route, or with the assistance of fluoroscopy.[7] Sonography and CT scans are also commonly employed for coracoid fracture diagnosis, with CT scans providing three-dimensional reconstruction and serving as the gold standard.
Conservative treatment involves immobilizing the shoulder followed by intensive physiotherapy to restore range of motion after the fracture has healed. Currently, there are no established surgical indications for type 2 fractures.[6] However, some physicians may consider surgical intervention in cases of painful non-union, displacement exceeding 1 cm, concurrent ipsilateral scapula fracture, a glenoid step of 4mm, medialization of the glenohumeral joint by 20mm, angular deformity of at least 25 degrees, or evidence of superior shoulder suspensory complex injury. [7] Coracoid fractures are often associated with injuries to the ribs, clavicle, lungs, and brachial plexus.[8]
Conclusion
In conclusion, it is crucial to carefully assess individuals who have experienced a direct shoulder impact or significant traction of the upper arm for potential isolated coracoid fractures. Performing specialized imaging such as scapula Y or axillary radiographs is essential to accurately visualize the entire length of the coracoid process and prevent the oversight, delay, or misdiagnosis of such fractures. Computed tomography (CT) scans with three-dimensional reconstruction are considered the preferred diagnostic modality for coracoid fractures. In cases of isolated undisplaced type I fractures and the majority of type II fractures, conservative treatment is recommended.
Declaration of Interests
No financial or non-financial support was received from public, commercial, or not-for-profit entities for this study.
Ethical Statement
The patient was informed about the technique and procedures involved in the study in her native language. Prior to publication, we obtained her consent to submit the article and accompanying photographs for publication.
Conflict of Interest
None.
Source of Funding
None.
References
- T Martín-Herrero, C Rodríguez-Merchán, L Munuera-Martínez. Fractures of the coracoid process: presentation of seven cases and review of the literature. J Trauma 1990. [Google Scholar]
- K Ogawa, A Yoshida, M Takahashi, M Ui. Fractures of the coracoid process. J Bone Joint Surg Br 1997. [Google Scholar] [Crossref]
- K Ogawa, N Matsumura, A Yoshida, W Inokuchi. Fractures of the coracoid process: a systematic review. JSES Rev, Rep, Techniques 2021. [Google Scholar]
- R Botchu, KJ Lee, S Bianchi. Radiographically undetected coracoid fractures diagnosed by sonography. Skeletal Radiol 2012. [Google Scholar]
- E Vaienti, F Pogliacomi. Delayed diagnosis of isolated coracoid process fractures: results of 9 cases treated conservatively. Acta Biomed 2012. [Google Scholar]
- A Güleç, H Kütahya, R G Göncü, S Toker. Isolated Fracture of the Coracoid Process. Case Rep Orthop 2014. [Google Scholar] [Crossref]
- J Anavian, CA Wijdicks, LK Schroder, S Vang, PA Cole. Surgery for scapula process fractures: Good outcome in 26 patients. Acta Orthopaedica 2009. [Google Scholar] [Crossref]
- RJ Imatani. Fractures of the scapula: A review of 53 fractures. J Trauma 1975. [Google Scholar] [Crossref]