
Introduction
Ankle and foot pain is a common condition in skeletally immature active children. Sport related and traumatic injuries are the most common causes of foot pain in children and adolescents.1, 2, 3 However several different etiologies can lead to ankle and foot problems with this young age group. Tarsal coalition, painful accessory bone, biomechanical problems and alteration of the endochondral ossification should be considered and excluded as the cause of persistent ankle pain.4 An accessory ossification center of the distal tibial epiphysis is located at the tip of the medial malleolus. It generally fuses to the tibial epiphysis with progressive skeletal growth. But, sometimes it may remain unfused below the malleolus.5 This accessory ossification center is asymptomatic in most of the cases and is only discovered incidentally by a radiograph of the ankle taken for some other ankle pathology. However, in some cases, it becomes fragmented and symptomatic, usually in children involved in sport activity. It is mostly unilateral but bilateral presentation is very rare. Exact etiology and pathogenesis is unknown. Some authors have postulated this symptomatic fragmentation of the accessory ossification center of the distal tibial epiphysis to a traction apophysitis of the medial malleolus caused by repetitive trauma during vigorous sport activity.6, 7 Other authors have reported cases with similar symptoms in which radiographic fragmentation of the entire distal tibial epiphysis was present and these cases were related to an ankle trauma or to congenital or neurological diseases. 8, 9, 10, 11, 12, 13, 14 Klein et al. reported the first case of osteochondrosis juvenilis of the medial malleolus, in which only the medial malleolus was fragmented, rather than the entire distal epiphysis of the tibia. 15 We are reporting a case of osteochondrosis of the accessory ossification center of the medial malleolus in a 9 years old girl in both ankle, with no history of trauma, fever or other joint diseases which was treated conservatively and completely resolved in eight months.
Case Report
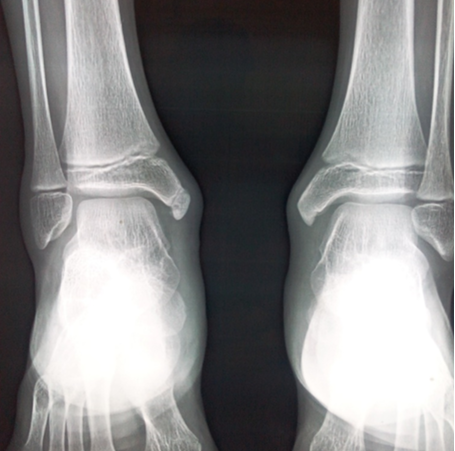
A 9 years old girl who presented with chief complaints of pain and swelling at the both medial malleoli. Pain was insidious in onset. Pain started without any traumatic events or sport injury. Pain was progressively increasing in intensity. Patient was evaluated at the MRA Medical College, Department of Orthopaedic Surgery, Ambedkar Nagar. There was no history of ankle trauma, fever, another joint pain or swelling. The patient was not involved in any sport activity. The pain became worse with activity and improved with rest and medications. On clinical examination, a mild swelling was present over the tip of the bilateral medial malleoli and palpation of the medial malleolus was tender on both side, local temperature not raised, the range of motion of the ankle joint and of the foot of both side was normal, but it was painful at the extreme degrees of foot pronation–eversion (Figure 1). On valgus stress there was pain in both medial malleoli. There was no gross foot deformity. No lower limb discrepancy or limb malalignment were observed. No history of trauma or ankle infection were reported. There was no other significant past history. Laboratory work-up for inflammatory disease and infections were within normal limit. The radiographs of both ankles showed accessory ossification center of the bilateral medial malleoli which was fragmented on both sides (Figure 2). On the basis of the clinical and radiological examination; and ruling out other possible differential diagnosis; we made a diagnosis of osteochondrosis of the accessory ossification center of the medial malleolus epiphysis. Treatment consist of reducing sport activity, hot saline fomentation and NSAIDS. The ankle pain and swelling progressively disappeared in 8 months. No cast or brace was used. Radiographic examination, performed 8 months after diagnosis, showed complete reconstruction of the accessory ossification center of the medial malleolus.

Discussion
Ankle pain is common in growing age group. There are some pathological conditions causing chronic pain in the medial malleolus during this period of skeletal growth, such as traction apophysitis of the medial malleolus, osteochondrosis, osteochondritis or avascular necrosis of the distal tibial epiphysis, neglected injury over medial malleolus leading to fracture of tip of medial malleolus nonunion or pseudoarthrosis or cartilaginous fracture. Osteochondrosis of acessory ossification center of medial malleolus is rare cause of ankle pain. Bilateral involvement is very rare. Due to rarity of this disease and similar presentation to other cause of ankle pain this is generally misdiagnosed. Osteochondrosis is a focal multifactorial breakdown of endochondral ossification in a region of previously normal endochondral growth. During childhood all ossification center are likely to develop osteochondrosis and a meticulous clinical examination is essential in the diagnostic process. Osteochondrosis of the medial malleolus epiphysis is a rare situation and few cases have been reported in literature. 6, 15, 16, 17 Medial malleolus can show an accessory ossification center as a normal variant in growing children. Sport activity could influence the formation of this accessory ossification center. The incidence of an accessory ossification center in the medial malleolus ranges from 1.6 to 47%.5, 18, 19, 20 This accessory ossification center appears at the tip of the medial malleolus at an average age of 7.6 years in girls and 8.7 years in boys and it is usually asymptomatic. 19 According to some authors the accessory ossification center of the medial malleolus may be present bilaterally or unilaterally but mostly unilateral and it is more frequent in girls and in children involved in sport activity.18, 19 There are lots of differential diagnosis for this pathological condition with similar clinical features and presentation in this age group. Tajima et al. compared ankle X-rays of 292 children of a junior football club to 124 control subjects. He reported an accessory center in 11.2% of young football players and in only1.6% of the control group. 20 This difference was due to the mechanical stress caused by a repetitive traction of the deltoid ligament during sport activity. Mechanical repetitive tractions of the deltoid ligament were indicated as a possible etiologic key factor to the accessory ossification center formation.6, 20 On the other hand, a recent study analyzed 550 ankle X-rays observing four specific developmental stages of the medial malleolus. La Mont et al. stressed the concept that secondary ossification center appears as part of a continuum of a development of the medial malleolus.21 Ogden and Lee reported that this painful condition caused by cartilaginous fracture, fibrous union or pseudoarthrosis, and recommended bone scintigraphy to make the diagnosis. 22 Ishii et al. and Gupta et al. underlined the importance of repetitive trauma at the medial malleolus, which is stressed by the deltoid ligament during sport activity in young athletes.6, 7 Local and systemic biochemical inflammatory activations, genetic predisposition, local ischemia, and mechanical alteration are etiological key factors in osteochondrosis pathogenesis.23 Mechanical excessive load on the medial epiphysis and repetitive micro trauma seems to be an important etiological role in this osteochondrosis as in Osgood-Schlatter’s disease and Sinding-Larsen-Johansson syndrome. 24 Osteochondrosis of the accessory ossification center of the bilateral medial malleolus is a rare entity.
In our case, the accessory ossification center became painful at 9 years of age, without any history of trauma. The patient did not engage in any specific sport such as to justify a traction apophysitis in the medial malleolus. There was no history of previous trauma so fracture of tip of medial malleolus, nonunion, pseudoarthrosis or cartilaginous fracture is ruled out. However, the accessory ossification center at radiographic examination was completely fragmented in both side, similar to that described by Klein et al. 15 Therefore, this pathological condition should be considered an osteochondrosis of the accessory ossification center of the medial malleolus of both sides. It was painful and fragmented, similar to the most common osteochondrosis present other site in the growing skeleton age group (Osgood–Schlatter, Sinding– Larsen–Johansson, Sever–Blanke).25 Follow-up after 8 months of the diagnosis, the patient was pain free and radiograph showed complete recovery from the disease with a perfect remodelling of the medial malleolus.
Conclusion
Osteochondrosis is characterized by a disturbance of enchondral ossification in skeletally immature patients. Ostochondrosis of accessory ossification center of bilateral medial malleoli is very rare entity but well recognized condition in clinical practice. Due to common age group and similar presentation with other differential diagnosis it should be consider in differential diagnosis in children having a history of persistent foot and ankle pain. By this we can reduce the number of missed cases.