- Visibility 140 Views
- Downloads 44 Downloads
- Permissions
- DOI 10.18231/j.ijor.2023.014
-
CrossMark

Expert opinions on the prevalence, diagnosis and treatment choice for osteoarthritis management in Indian settings
- Author Details:
-
 Manjula S *
Manjula S *
-
Krishna Kumar M
Abstract
Background: Studies have reported the capability of bisphosphonates to delay the progression of structural deterioration associated with osteoarthritis (OA). Limited studies exist regarding OA management in India and the determinants influencing patients' decisions regarding surgical interventions. So, this study aimed to assess the prevalence, diagnostic practices, and treatment options available for OA management in Indian clinical practice with a special focus on alendronate, a bisphosphonate medication for OA pain management.
Materials and Methods: The cross-sectional, multiple-response questionnaire-based study collected a survey response using a 25-item questionnaire from 276 clinicians across India. Additionally, the survey focused on determining the diagnostic practices helpful in determining osteoporosis and the preference of treatment options for OA management.
Results: Based on the responses of 276 participants, 43% indicated that the diagnosis of OA was predominant in both genders. Moreover, about 51% of the respondents suggested that mass screening for osteoporosis in Indian patients should be conducted using the one-minute risk test developed by the International Osteoporosis Foundation. Additionally, 47% of the respondents highlighted hip fractures as the most common type of bone fracture observed in these patients. Furthermore, around 51% of the study participants emphasized that adequate calcium consumption during childhood can potentially reduce the incidence of osteoporosis. For the effective management of OA, alendronate was preferred by 49% of respondents over the other bisphosphonates.
Conclusion: As per the expert consensus, patients who have osteoporosis risk factors and osteopenia without fragility fractures were recommended to adhere to dietary and lifestyle modifications, coupled with calcium and vitamin D supplementation, and bisphosphonate therapy. Alendronate was preferred over other bisphosphonates for the effective management of OA.
Introduction
Osteoarthritis (OA) is the seventh most common disease worldwide and accounts for 15% of all musculoskeletal conditions. India has a higher global rate of OA proliferation and is projected to lead the world in chronic diseases by 2025.[1] About 365 million people worldwide have OA, with the knee joint being the most commonly affected followed by the hands and hip.[2] The diagnosis of OA was primarily based on radiodiagnosis and clinical symptoms. Moreover, recent advancements in diagnostic methods, including innovative imaging modalities and biochemical assessments, have contributed to a broader understanding of the condition. These advancements have enabled the evaluation of all the essential components of joint tissue more comprehensively.[3]
In North America, the primary focus of knee OA treatment was symptom management and enhancing knee function to prevent further progression and the need for knee replacement surgery.[4] Apart from active treatments (like physical therapy, exercises, orthotics, or manual therapy focused on improving strength and mobility), treatment usually involves a combination of pharmaceutical interventions (such as analgesics and anti-inflammatory agents), natural supplements, and intra-articular injections of corticosteroids or hyaluronic acid.[4]
Bisphosphonates are primarily used to treat osteoporosis due to their potential in preventing osteoclast-mediated bone loss, and there was ample literature evidence to support their clinical use. Studies have also reported the capability of alendronate and tiludronate to delay the progression of structural deterioration associated with OA. [5], [6] Similarly, a clinical investigation revealed that the use of bisphosphonates, including ibandronate, pamidronate, risedronate, and zoledronate, was associated with a 26% lower incidence of knee replacement in older women.[7]
The data from the 2014 Osteoarthritis Initiative reported alendronate as the most commonly used bisphosphonate (>60%) and noted a significant reduction in the numeric rating scale, during the initial 3 years of using bisphosphonates. The study also observed a decline in effects by the fourth year and attributed this to probable reduced adherence or compliance. [8] Joint space narrowing was also found to be decreased over time in individuals receiving bisphosphonates. Alendronate has been reported to delay disc space narrowing and the progression of spinal osteophytes, suggesting its potential to slow down the advancement of spinal osteoarthritis.[9]
Further new studies are imperative to outline the precise indications and ideal course of alendronate treatment due to the lack of large-scale, randomized, and double-blind trials that address this issue. Limited studies exist regarding OA management in India and the determinants influencing patients' decisions regarding surgical interventions. In an effort to bridge this gap, the present survey aims to assess the prevalence, diagnostic practices, and treatment strategies adopted by clinicians for OA management.
Materials and Methods
We carried out a cross sectional, multiple-response questionnaire based survey among clinicians specialized in treating OA and osteoporosis patients in the major Indian cities from June 2022 to December 2022.
Questionnaire
The questionnaire booklet titled CORE (Comprehensive Osteoporosis and osteoaRthritis Evaluation) study was sent to the physicians who were interested to participate. The CORE study questionnaire focused on the diagnosis, clinical characteristics of patients with OA, and available treatment options. The study was conducted after receiving approval from Bangalore Ethics, an Independent Ethics Committee which was recognized by the Indian Regulatory Authority, Drug Controller General of India.
Participants
An invitation was sent to leading clinicians in managing OA and osteoporosis in the month of March 2022 for participation in this Indian survey. 276 doctors from major cities of all Indian states representing the geographical distribution shared their willingness to participate and provide necessary data. Physicians were asked to complete the questionnaire without discussing with peers. A written informed consent was obtained from each clinician’s prior initiation of the study.
Statistical analysis
Descriptive statistics was used to analyze the data. Categorical variables were represented by percentages. A frequency and percentage distribution were used to present each variable's distribution. Excel 2013 (16.0.13901.20400) was used to generate pie chart.
Results
Based on the responses obtained from 276 participants, 41% of them reported that the prevalence of OA diagnosis was highest among individuals aged 40-49 years. About 44% of the participants noted that OA diagnosis was predominantly associated with females, while an equivalent percentage (43.47%) reported that both genders were commonly diagnosed with OA. Furthermore, 38% indicated that approximately 21-40% of patients with OA were obese, while 36% of them indicated that 21-30% of OA patients have a comorbid osteoporosis condition.
Around 51% of the respondents stated that the International Osteoporosis Foundation's (IOF) one-minute risk test was most effective for mass osteoporosis screening in Indian patients. Out of the 276 participants, 47% of them indicated that hip fractures were the most commonly observed type of bone fracture among patients with osteoporotic fractures. Additionally, about 29% and 30% of the respondents indicated that upper limb fractures and spine fractures, respectively, were the most frequently observed types of bone fractures among patients with osteoporotic fractures.
Approximately half of the study participants (50.72%) reported that sufficient intake of dietary calcium during childhood can decrease the risk of osteoporosis. Nearly 41% of the respondents stated that dietary calcium supplementation might play a role in reducing the risk of fractures. Furthermore, around 38% of the respondents indicated that 11-20% of newly diagnosed patients with OA required joint replacement surgery.
Approximately 54% of participants concurred that complementary and alternative medications were beneficial in managing OA pain, while 45% of them disagreed and did not favour complementary and alternative medicine for OA management. The preferred options for OA management were the use of calcium or collagen supplements, calcium carbonate, initial avoidance of surgery, and physiotherapy ([Table 1]).
|
Preference for complementary and alternative medications to manage OA pain |
Response rate (n=276) |
|
Yes |
150 (54.34%) |
|
No |
125 (45.28%) |
|
Not attempted |
1 (0.36%) |
|
Others |
|
|
Calcium supplements |
2 (0.72%) |
|
Collagen supplements |
5 (1.81%) |
|
Initial avoidance of surgery |
1 (0.36%) |
|
Physiotherapy |
1 (0.36%) |
|
Use of calcium carbonate for OA pain |
1 (0.36%) |
Approximately 43% of participants expressed that utilizing ultrasound to measure bone mineral density was beneficial for mass screening of patients at risk of osteoporosis. Additionally, 35% of the participants identified it as the most reliable tool for diagnosing osteoporosis ([Table 2]).
|
Measuring bone mineral density by ultrasound in the diagnosis of osteoporosis |
Response rate (n=276) |
|
As it does not measure bone mineral density directly, it cannot be used to diagnose osteoporosis |
58 (21.01%) |
|
It is a reliable and cheaper technique to diagnose osteoporosis |
96 (34.78%) |
|
It is a useful tool for mass screening of the population at risk, who need further investigation |
118 (42.75%) |
|
It is useful only in post-menopausal women |
6 (2.17%) |
A total of 45% of respondents recommended nutritional and lifestyle modifications, along with treatment involving calcium and vitamin D supplements, as well as bisphosphonates for patients who exhibited risk factors for osteoporosis and possessed a T-score ranging between -1 and -2.5 (osteopenia) without fragility fractures. Furthermore, 34% of them reported suggesting calcium and vitamin D treatment for these patients with risk factors and indications of osteopenia, all without fragility fractures ([Table 3]). In terms of follow-up recommendations, over half of the respondents (52.17%) proposed repeating the dual-energy X-ray absorptiometry (DEXA) scan once annually for patients with a T-score ranging from -2 to -2.4. In contrast, 38% of the participants advised conducting this DEXA scan for these patients once every two years ([Table 4]).
|
Clinicians’ advice for patients with risk factors and a T score between -1 to -2.5 (osteopenia) without fragility fractures |
Response rate (n=276) |
|
Nutritional and lifestyle modifications |
37 (13.40%) |
|
Treatment with calcium and vitamin D |
95 (34.42%) |
|
Treatment with bisphosphonates |
28 (10.14%) |
|
All the above |
125 (45.28%) |
|
Recommendation on repeat DEXA scan for patients with T-score of -2 to -2.4 |
Response rate (n=276) |
|
Every 1 year |
144 (52.17%) |
|
Every 2 year |
104 (37.68%) |
|
Every 5 year |
27 (9.78%) |
|
Others |
1 (0.36%) |
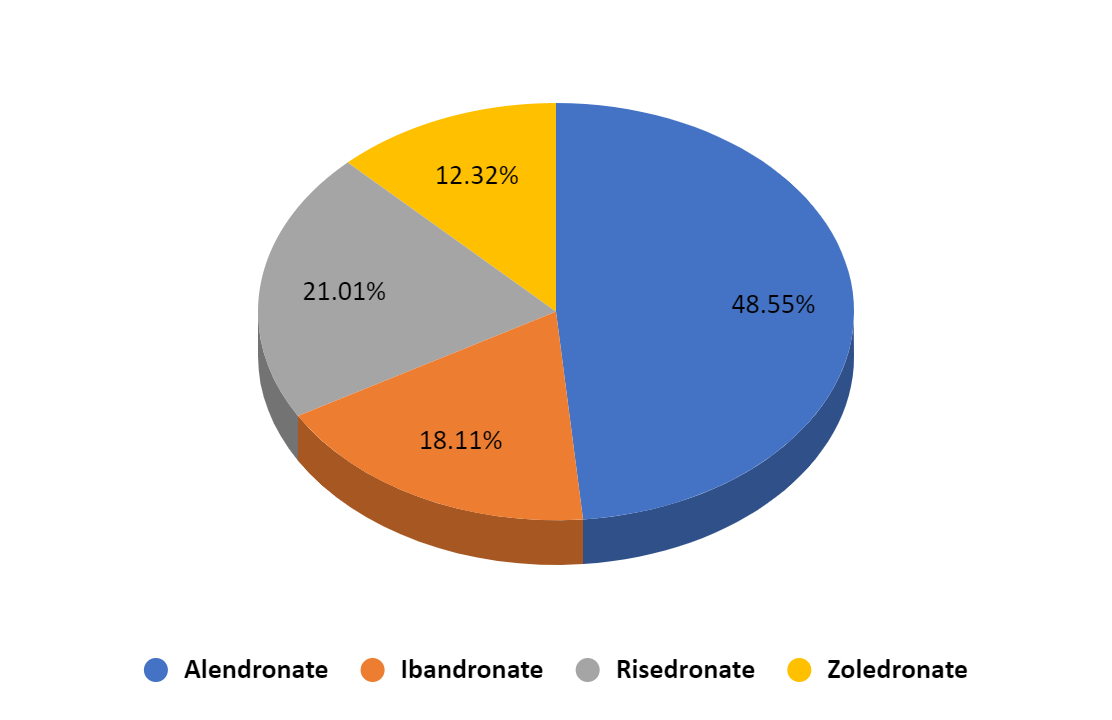
Approximately 66% of participants reported that non-steroidal anti-inflammatory drugs, physiotherapy, diet, and exercise play a major role in the early management of OA ([Table 5] ). Regarding patients with osteoporosis, about 49% of the respondents recommended alendronate, while 21% of them suggested risedronate as part of bisphosphonate treatment ([Figure 1] ).
|
Preference towards the early management of OA |
Response rate (n=276) |
|
Non-steroidal anti-inflammatory drugs |
28 (10.14%) |
|
Physiotherapy |
38 (13.76%) |
|
Diet and exercise |
36 (13.04%) |
|
All the above |
181 (65.58%) |
Discussion
The survey involving 276 participants revealed that OA was more prevalent among females and both males, with the condition being particularly common in individuals aged between 40-49 years. Additionally, expert opinions indicated that 21-40% of patients are obese and have been reported to exhibit a comorbid osteoporosis condition. The Beijing Osteoarthritis Study has identified a more prevalent occurrence of knee OA among Chinese women and older individuals aged ≥70 years. Additionally, the prevalence of knee OA in Chinese men was found to be comparable to their white US counterparts in terms of both radiological and symptomatic OA. [10] Cross et al. has also indicated a higher global age-standardized prevalence of knee OA at 3.8% in females than males. [11] On a global scale, it is projected that the prevalence of osteoarthritis will continue to rise due to aging populations, increasing obesity and injury rates, and other contributing factors.
A notable number of respondents indicated that the IOF one-minute risk test was most effective in Indian patients for mass osteoporosis screening. A study by Lin et al. employed IOF one-minute risk test and identified age, education level, results of bone density test, previous disease diagnosis, long-term drug use, physical fitness, dietary habits, and average time spent in the sunlight as the factors to considered as a risk for osteoporosis. [12] As per a significant proportion of respondents in the current study, the joint most frequently affected among osteoporotic subjects was the hip, followed by upper limb and spine fractures. This was consistent with the findings of Anandacoomarasamy and March, who reported that knee, hip, cervical and lumbar spine, distal interphalangeal, proximal interphalangeal, carpometacarpal, and metatarsophalangeal joints were the most commonly affected joints in cases of OA. [13]
More than half of the experts suggested that the impact of osteoporosis and fracture risk can be reduced through adequate dietary calcium supplementation during childhood. For optimal therapy, patients with bone loss should continue to receive adequate calcium and vitamin D. However, it is concerning that over 50% of women undergoing treatment for bone loss have insufficient vitamin D levels, and more than 90% of women might not be obtaining adequate calcium intake. [14] There were already a number of pharmacologic therapies for osteoporosis that increase bone mass and lower the risk of fracture. When enough calcium and vitamin D supplementation was attained, several treatments have been evaluated.
As per the responses from the current study participants, strategies such as initial avoidance of surgery, physiotherapy, collagen supplements, calcium supplements, and the utilization of calcium carbonate were preferred for managing OA pain. Notably, a significant number of respondents suggested these approaches for addressing the discomfort associated with OA. In addition, prominent respondents provided guidance to patients displaying risk factors for osteoporosis and possessing a T-score ranging between -1 and -2.5 (osteopenia) without fragility fractures. The recommended measures included adopting dietary and lifestyle changes, incorporating calcium and vitamin D supplements, and considering the use of bisphosphonates as part of the management plan. Among the bisphosphonate treatments, alendronate and risedronate were recommended by the majority of the experts participating as effective options for patients with osteoporosis.
Consistent with these findings, a prospective open-label study has concluded that alendronate reduces pain and disability scores (P <0.001) in 41 patients treated for avascular necrosis of the hip. [15] A mice model study by Evans et al. investigated the role of alendronate in osteogenesis imperfecta. According to their findings, high doses of alendronate prevent mice from growing long bones by altering the growth plate and possibly reducing the resorption of the chondro-osseous junction. [16] Furthermore, Nishii et al. observed that a two-year consumption of alendronate was effective in alleviating pain, particularly when there were no notable changes in OA as indicated by radiographic joint space width. [17] Additionally, Hu et al. reported there was a possibility that alendronate contributes to the relief of OA-associated pain by suppressing matrix metalloproteinase-13, a cytokine. [18] Collective evidence from both in vitro and clinical studies suggested that alendronate treatment at the recommended dosage provides clinical benefits in terms of pain reduction. However, these studies did not show any protective effects against the structural progression of hip osteoarthritis.
The current survey findings focusing on the prevalence and diagnosis of OA and the significance of alendronate for managing OA pain offer valuable insights for making well-informed decisions to achieve optimal treatment results for patients with OA. However, it was important to acknowledge that the current study has certain limitations. The potential for widespread applicability of the results might be restricted due to the study's relatively small sample size. Given that the conclusions were based on expert opinions, there was a possibility that inherent biases or individual perspectives could influence the interpretations drawn from the data. This should be taken into consideration when interpreting and applying the survey's results in clinical practice.
Conclusion
According to the consensus among experts, individuals with risk factors for osteoporosis and a T score ranging from -1 to -2.5 (osteopenia), but without fragility fractures, were advised to undergo dietary and lifestyle modification, alongside the incorporation of calcium and vitamin D supplementation, and the use of bisphosphonate therapy. Among the range of bisphosphonates available, alendronate was favoured over others for the efficient management of OA.
Source of funding
None.
Conflict of Interest
None.
Acknowledgement
We would like to thank all the clinicians who were participated in this study.
References
- Azad C, Singh A, Pandey P, Singh M, Tia N, Rastogi A. Osteoarthritis in India: An epidemiologic aspect. Int J Recent Sci Res. 2017;8(10):20918-22. [Google Scholar]
- Long H, Liu Q, Yin H, Wang K, Diao N, Zhang Y. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: Findings from the global burden of disease study 2019. Arthritis Rheumatol. 2022;74(7):1172-83. [Google Scholar]
- Kuyinu E, Narayanan G, Nair L, Laurencin C. Animal models of osteoarthritis: classification, update, and measurement of outcomes. J Orthop Surg Re. 2016;11(1). [Google Scholar] [Crossref]
- Das S, Farooqi A. Osteoarthritis. Best Pract Res Clin Rheumatol. 2008;22(4):657-75. [Google Scholar]
- Moreau M, Rialland P, Pelletier J, Martel-Pelletier J, Lajeunesse D, Boileau C. Tiludronate treatment improves structural changes and symptoms of osteoarthritis in the canine anterior cruciate ligament model. Arthritis Res Ther. 2011;13(3). [Google Scholar] [Crossref]
- Panahifar A, Maksymowych W, Doschak M. Potential mechanism of alendronate inhibition of osteophyte formation in the rat model of post-traumatic osteoarthritis: evaluation of elemental strontium as a molecular tracer of bone formation. Osteoarthritis Cartilage. 2012;20(7):694-702. [Google Scholar]
- Neogi T, Li S, Peloquin C, Misra D, Zhang Y. Effect of bisphosphonates on knee replacement surgery. Ann Rheum Dis. 2018;77(1):92-7. [Google Scholar]
- Laslett L, Kingsbury S, Hensor E, Bowes M, Conaghan P. Effect of bisphosphonate use in patients with symptomatic and radiographic knee osteoarthritis: data from the Osteoarthritis Initiative. Ann Rheum Dis. 2014;73(5):824-30. [Google Scholar]
- Neogi T, Nevitt M, Ensrud K, Bauer D, Felson D. The effect of alendronate on progression of spinal osteophytes and disc-space narrowing. Ann Rheum Dis. 2008;67(10):1427-30. [Google Scholar]
- Zhang Y, Xu L, Nevitt MC, Aliabadi P, Yu W, Qin M. Comparison of the prevalence of knee osteoarthritis between the elderly Chinese population in Beijing and whites in the United States: The Beijing Osteoarthritis Study. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 2001;44(9):2065-71. [Google Scholar]
- Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M. The global burden of hip and knee osteoarthritis: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(7):1323-30. [Google Scholar]
- Lin L, Lai W, Hsu S, Lin J. Early Osteoporosis Risks and Associated Factors among Caregivers Working in Disability Institutions: IOF One-Minute Osteoporosis Risk Check. Int J Environ Res Public Health. 2020;17(9). [Google Scholar] [Crossref]
- Anandacoomarasamy A, March L. Current evidence for osteoarthritis treatments. Ther Adv Musculoskelet Dis. 2010;2(1):17-28. [Google Scholar]
- Holick MF, Siris ES, Binkley N, Beard MK, Khan A, Katzer J. Prevalence of Vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J Clin Endocrinol Metab. 2005;90(6):3215-24. [Google Scholar]
- Agarwala S, Jain D, Joshi VR, Sule A. Efficacy of alendronate, a bisphosphonate, in the treatment of AVN of the hip. A prospective open-label study. Rheumatology. 2005;44(3):352-9. [Google Scholar]
- Evans K, Lau S, Oberbauer A, Martin R. Alendronate affects long bone length and growth plate morphology in the oim mouse model for Osteogenesis Imperfecta. Bone. 2003;32(3):268-74. [Google Scholar]
- Nishii T, Tamura S, Shiomi T, Yoshikawa H, Sugano N. Alendronate treatment for hip osteoarthritis: prospective randomized 2-year trial. Clin Rheumatol. 2013;32(12):1759-66. [Google Scholar]
- Hu H, Zhang L, Li B, Zhang Y, Liu X, Tian F. In vitro effect of alendronate on chondrocytes and articular cartilage and subchondral bone in rabbit anterior cruciate ligament transection model. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2009;23(12):1474-81. [Google Scholar]